![]()
Writings on Malaria |
A Study of a Malaria Epidemic - Guadalcanal Weather Coast
The distribution of cases
The map shows part of the Weather Coast of
Guadalcanal and the names of villages in which Plasmodium vivax
cases were detected during 1972. The numbers of cases and the months in
which they were detected also are shown.
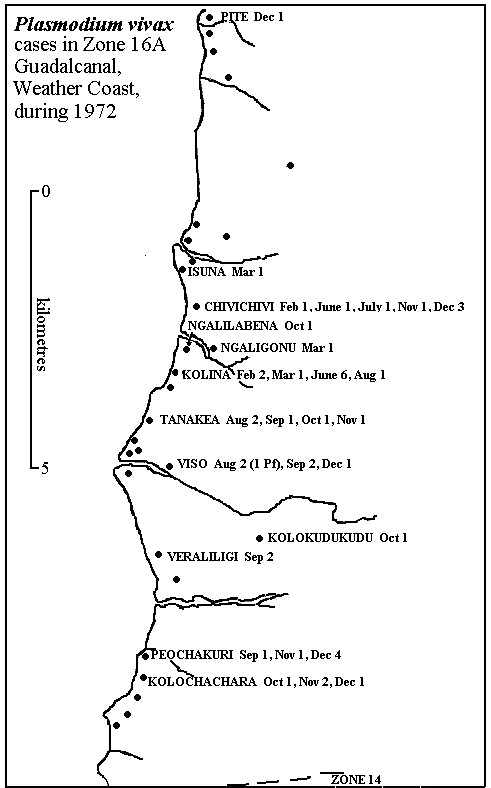
You will see that the earliest cases in the year were in two villages, Chivichivi and Kolina, during February. As the year went by the number of cases detected and the spread of the cases gradually increased. It is worth noting that during the months of January, April and May there were no slides collected anywhere in the Zone (Zone 16A).
Towards the end of the year the malaria level was at its highest point for many years. Why did this happen?
The cause of the epidemic
The major reason for the increase in the malaria transmission was that the only cyclical spraying operation during the year was in February, Due to a shortage of DDT it was not possible to spray this Zone in August and as the spraying schedule was badly delayed it was decided to miss out the Weather Coast Zones.
However, the breakdown in spray coverage is not the source of the epidemic, what we have to ask is where did the epidemic start?
Looking at our village case record cards we can find the answer.
(a) At Kolina in 1971 there were two cases, one of these was Basili, aged 3. In February 1972, the first case of the year was Basili Balua aged 4.
(b) At Chivichivi the record card reads as follows;
| Date slide taken | Name of patient | Age of patient | Notes |
| 15 Sept 1971 | Wate Kali | 61 | |
| 15 Sept 1971 | Silas Saikelana | 4 | |
| 15 Sept 1971 | Henry Watekali | 2 | |
| 28 Sept 1971 | Rosa Perotogha | Ad. | |
| 3 Feb 1972 | Silas Saikalana | 4 | FUC slide |
| 22 June 1972 | Ki-Tora | 4 | |
| 16 July 1972 | Silas Saikalana | 4 | |
| 21 Nov 1972 | Willy Patilevu | 1 | |
| 6 Dec 1972 | Bethel Dueli | 4 | |
| 19 Dec 1972 | Henry Watekali | 6 | |
| 19 Dec 1972 | Ki-Tora | 4 | FUC slide |
You can see that at both of these villages the first cases of 1972, and probably the cause of the epidemics, was a relapse in a four year old child. Poor Silas at Chivichivi had a second relapse in July. Also at Chivichivi two other names appear twice, Henry Watekali and Ki-Tora.
Conclusion
It is clear from these records that it is a young child that is most likely to relapse and in this epidemic only 5 of the 44 cases were over eight years old. The age group around four to six is undoubtedly the most difficult to treat but you can see how important it is that all cases receive full radical treatment.
What may have added to this epidemic was that the February cases were not investigated until mid-March (and probably radical treatment was not started until then) and the March cases were not investigated until the end of June.
You will remember as well that in the case of a vivax relapse gametocytes can appear right away at the start of the relapse and so transmission is possible straight away.
This epidemic spread because of the long overdue spraying but would not have started if the patients had received proper radical treatment when their malaria was first detected.
I hope this study of a malaria epidemic will help to remind all the Supervisors and Senior Malaria Technicians what can happen in their Regions. The Western District is now, we hope, in its last year before entering Consolidation and if we cannot find and treat all malaria cases we will lose the battle.
Dr. B. Taylor
13.2.73
![]()
| ©1999 - Brian Taylor CBiol FIBiol
FRES 11, Grazingfield, Wilford, Nottingham, NG11 7FN, U.K. Visiting Academic in the Department of Life Science, University of Nottingham Comments to dr.brian.taylor@ntlworld.com |
href="\malaria\malaria5.htm"